Hydroxychloroquine does not reduce deaths from COVID-19 and may even cause unwanted damage, recent studies have found. According to the new Cochrane Review, the drug probably does not reduce the number of people needing mechanical ventilation.
“In addition, they note that no new trials of hydroxychloroquine or chloroquine for treating COVID-19 should be started,” the South African Medical Research Council (SAMRC) said on Tuesday. The findings are contained in the study published by authors based in India, South Africa, and the United Kingdom, who undertook the systematic review of studies that used chloroquine or hydroxychloroquine for treating or preventing COVID-19 disease.
It is also likely that hydroxychloroquine caused more unwanted effects than placebo in the trials undertaken. I think this underlines the importance of ensuring that we have reliable evidence even in an emergency situation like this pandemic where there is public pressure for rapid treatments and prevention options.
Dr Tamara Kredo, Cochrane South Africa, SAMRC
“They searched for studies that examined giving chloroquine or hydroxychloroquine to people with COVID-19; people at risk of being exposed to the virus; and people who had been exposed to the virus,” the SAMRC explained. According to the SAMRC, the public demand for a COVID-19 cure fuelled speculation that the drug might be effective based on unreliable research that did not meet the inclusion criteria of this review.
“The then US President Trump declared chloroquine a ‘game changer’ about a year ago, leading to global demand and confusion. The research community rapidly organised large trials, which demonstrated no evidence of an effect, and these trials are summarised in this review.”
The Council said the review authors included 14 relevant studies of which 12 were studies of chloroquine or hydroxychloroquine used to treat COVID-19 in 8 569 adults. Meanwhile, the two studies focused on whether hydroxychloroquine prevents COVID-19 in 3 346 adults who had been exposed to the virus but had no symptoms of infection. This included research from different countries, four in China and one each from Brazil, Egypt, Iran, Spain, Taiwan, the United Kingdom and North America and a global study in 30 countries.
According to the local author from Cochrane South Africa, Tamara Kredo, this review offers conclusive evidence that hydroxychloroquine has no impact on clinically important outcomes for both the prevention and treatment of COVID-19.
Senior author, Dr Tom Fletcher, said: “The review should put a line under using this drug to treat COVID-19. But some countries and health providers are still caught up in the earlier hype and prescribing the drug. We hope this review will help these practices end soon”. This Cochrane Review was co-ordinated by the Cochrane Infectious Diseases Group (CIDG), which has its editorial base at Liverpool School of Tropical Medicine (LSTM).
Cochrane South Africa (SA) is an internal research unit of the SAMRC and is part of the global, independent Cochrane network of researchers, professionals, patients, carers and people interested in health. Cochrane is a non-profit organisation that prepares and disseminates information on what works and what does not in healthcare. These reviews enable policymakers, health service providers and the public to make informed decisions about healthcare.
President of the European Commission, Ms Ursula von der Leyen, Director-General of the WHO, Dr Tedros Adhanom Ghebreyesus, CEO of Global Citizen, Mr Hugh Evans, Global Citizens and Friends,
South Africa is honoured once again to lend our support to Global Citizen, and to this Recover Better Together campaign. For the past 10 years, Global Citizen has been a leading voice for the involvement of governments, world leaders, philanthropists, activists, artists and the citizens of the world in ending extreme poverty.
When the coronavirus pandemic struck last year, Global Citizen responded swiftly, hosting the ‘One World: Together At Home’ benefit concert in support of healthcare workers on the frontline. The substantial pledges made for coronavirus relief at this event enabled NGOs around the world to help those most vulnerable.
The campaign we are launching today recognises that overcoming the COVID-19 pandemic is essential if we are to make any progress in tackling poverty. To achieve this, we must deepen cooperation to ensure equitable access to vaccines.
No person, no country and no region must be left behind. To fight the pandemic, we need to pool resources, capabilities, knowledge and intellectual property.
That is why we continue to call on world leaders to support the COVAX facility to ensure rapid and equitable access to COVID-19 vaccines for all countries. Applaud President Macron and EU that wealthier countries should donate 5% of their purchased vaccine stock to developing countries.
Another important step is to enable the transfer of medical technology for the duration of the pandemic. This will allow us to increase the production of COVID-19 vaccines and other medical products, lower prices and improve distribution to reach all corners of the world .
Alongside these efforts to overcome the pandemic, we must work together to end hunger, promote education and the resumption of learning, and protect the planet. By doing so, we will be contributing to a fair, just and inclusive recovery. The world will recover, it will recover better, and it will recover together. For the benefit of all leaving no one behind.
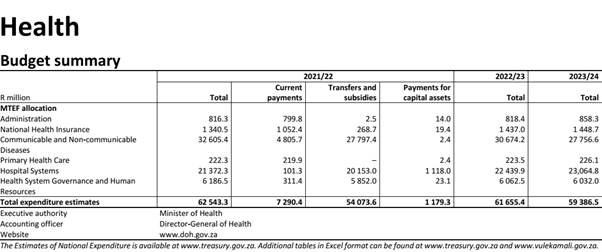
Government will in the next financial year avail an additional R8 billion to the health system for the country’s COVID-19 pandemic response.
This will be in addition to the R20 billion the state allocated in the 2020/21 financial year, Finance Minister Tito Mboweni said on Wednesday, while delivering the 2021 Budget Speech, in Parliament.
In a Budget Review document, the National Treasury said the funds were to enable the sector to expand prevention, screening, testing and hospital capacity.
The R8 billion, which will be allocated to provincial health departments through the provincial equitable share, is expected to enable the sector to sustain these activities and respond to possible future waves of COVID-19 infection.
“Provincial governments receive an additional R8 billion in 2021/22 to continue the public health response to the pandemic, and the potential for additional waves of infection. Provinces can mitigate the negative impact of COVID-19 and the associated lockdowns on their revenues by improving efficiency, particularly in the procurement of health equipment,” said the Minister.
In total, the health expenditure function will over the medium term make up 14.2 percent of total government spending, declining from R247 billion in 2020/21 to R245 billion in 2023/24.
“Provincial health departments receive about 92 percent (R678.7 billion) of these medium-term allocations.
Reductions to the sector, mostly focused on compensation spending, are estimated at about R50.3 billion over the 2021 MTEF period,” the document reads.
To achieve this, other reductions would be required from health departments to increase efficiency. This included generating savings through centralised procurement of certain goods, reducing variations in unit costs in HIV programmes and improving management of overtime costs.
The COVID-19 pandemic has had a massive impact on the South African health system. As at 16 February 2021, the country had 1.5 million confirmed cases and over 137 000 excess deaths as reported by the South African Medical Research Council.
Over the MTEF period, R29.4 million is allocated to Tygerberg Regional Hospital and R100 million to Klipfontein Regional Hospital in the Western Cape through the health facility revitalisation grant.
The timeline on NCDs policy development since 2011 with global and national contextual indicators. Its purpose is to show progress on policy developments and will be used as the basis for an advocacy tool. Please make your input and let us have feedback.
WHO is conducting an informal consultation of people living with diabetes about the Global Diabetes Compact. Online between 9-11 March 2021. SAST 14:00- 16-30
If you want to participate, apply here. There are a limited number of places so if you want to participate you need show your interest.
Better late than never. And it is only until October last year. Comorbidities are published once and not routinely by NICD. Oh now, the second wave is over “we will publish another list.” Really?
This requires some myth-busting action from the National Department of Health. I am tired of the comorbidities listed in media interviews by NDoH officials as going in this order: HIV, TB and more recently malaria (really). Then perhaps diabetes…. take a look and weep. Shame
Day One of the first phase of COVID-19 the vaccine rollout to health workers was a huge success today. South Africa secured the single-dose Johnson & Johnson (JnJ) vaccine for use in the Sisonke (‘Together’) programme. Sisonke will be rolled out to up to 500,000 healthcare workers starting in 18 public sector hospitals across all nine provinces.
As a demonstration of confidence in the safety and efficacy of the vaccine leaders from organised labour took their shots at Steve Biko Academic Hospital today. These are leaders who are health workers themselves from organisations like DENOSA, HOSPERSA, NEHAWU, NAPSU, NUPSAW and others.
Protecting our healthcare workers is an urgent priority
Phase 1 of the vaccine programme is focused on healthcare workers. This is the first step in rolling out a comprehensive vaccine distribution strategy for the nation. Healthcare workers are the frontline of the country’s COVID-19 response and are 3-4 times more likely to contract COVID-19 than the general population. To date 40,000 South African health workers have contracted COVID-19, 6,473 have been hospitalised and 663 of our colleagues have passed on.
Phase 1 of South Africa’s three phase vaccine rollout strategy was paused temporarily earlier this month following concerns regarding the efficacy of the Oxford-AstraZeneca (also known as CoviShield) vaccine against mild-moderate COVID caused by the 501.V2 variant. CoviShield may still play a role in the National Programme. However, more research is needed to determine how and when it will be used. Vaccination using a safe and efficacious vaccine must start without delay to protect healthcare workers during a likely 3rd wave this winter. The switch to the JnJ vaccine allows for the country to restart Phase 1 vaccine rollout to keep our health workers safe.
Single-dose JnJ vaccine
The single-dose JnJ vaccine protects against severe COVID-19 in South Africa. The safety and efficacy of the vaccine was assessed in the international Phase 3 study, ENSEMBLE, which was conducted across Latin America, USA and South Africa with more than 43 000 participants. South Africa contributed around 7,000 participants to the trial between October 2020 and February 2021, including participants who were exposed to the 501.V2 variant. The long-term follow-up of study participants is still ongoing, as is required for the process of regulatory approval by the South African Health Products Regulatory Authority (SAHPRA) for commercial or emergency use. However, since the safety and efficacy of the vaccine has already been proven, the current rollout is being conducted under The Sisonke Open Label Program, to assess real world effectiveness among health care workers, who have already been prioritised for vaccination by the South African Government’s Covid-19 Vaccination Strategy.
The JnJ vaccine has been shown to be safe, with no safety concerns reported from past trials or rollouts. The ENSEMBLE trial showed excellent protection of a single-dose vaccine against severe COVID-19, including in South Africa, and as such a delay in rolling out the vaccine would be unethical.
There is a clear process for vaccine rollout to healthcare workers. To receive the vaccine, healthcare workers must: (1) register on the South Africa Electronic Vaccination Data System, (2) respond to an SMS invitation, and (3) provide informed consent to take part. Healthcare workers will receive a vaccination voucher and communication once a vaccination centre is open to render the service. To register use this link: https://vaccine.enroll.health.gov.za/#/
The Sisonke rollout will include meaningful collaboration between the original team who were involved in the ENSEMBLE trial, JnJ, and the NDoH and the SAMRC. The partners will closely monitor, track and assess the real-world rollout of the vaccine. They will measure: (1) the occurrence of hospitalizations and deaths, (2) the incidence of severe SARS CoV-2 infections, (3) the diversity of breakthrough infections; and (4) evaluate vaccine uptake among healthcare workers in South Africa.
This experienced team will utilise their trained and qualified staff including pharmacists, clinicians and others to receive, store and oversee the dispensation of the JnJ vaccine. Sisonke staff will work very closely with national and provincial health public and private vaccine centres to ensure that the vaccination of healthcare workers is done safely and carefully managed.
The protection of our healthcare workers through the rollout of the safe and efficacious vaccine is an urgent priority for South Africa.
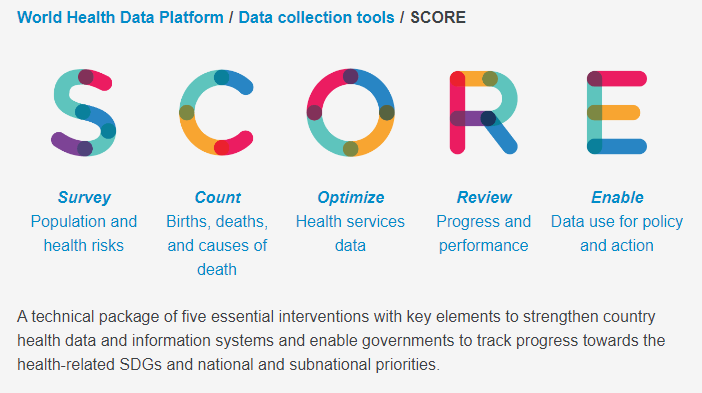
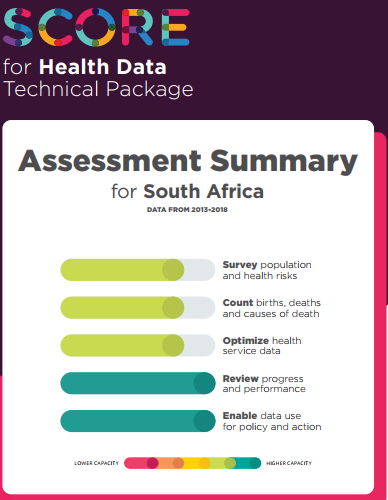
The SCORE for Health Data Technical Package represents the most comprehensive strategies and interventions for strengthening country health information systems. First launched in August 2020, it is a one-stop solution to improve the availability of timely, reliable and comparable health data to track progress towards the Triple Billion targets and health-related Sustainable Development Goals.
SCORE is the first time that all elements comprising an optimum health information system – Survey, Count, Optimize, Review, Enable – are captured in a single, harmonized package.