Early in the COVID-19 pandemic WHO’s @DrTedros highlighted the problems of access to health services by millions of people living with NCDs+ in his tweet. His tweet certainly mirrors what the SA NCDs Alliance and our allies have been saying since 2007 when the SA Human Rights Commission (SAHRC) held its first public hearings into the right access to health services.
COVID-19 changed the parameters of vulnerability to include NCDs+, mental health, and reemphasised disability in all its shapes and forms.
SAHRC report 2007
15 years ago the primary focus was understandably on access to HIV/AIDS and TB services. It was the height of the communicable disease epidemic. And amidst our homegrown “AIDS-denialism”. It was also the midpoint of the Millenium Development Goals (MDGs) where vast amounts of funding were channelled into communicable diseases and maternal-child services. That pattern of expenditure and funding remains in place today.
Executive summary
The report’s executive summary is salutary: it fits today’s health service access issues in the COVID-19 pandemic. Just substitute NCDs+ for communicable diseases. And, we have a similar complaint today.
The report’s opening quote is ironically, but not surprisingly, from The AIDS Law Project, the early version of Section 27:
“We don’t yet have a definition of essential health services. This means we don’t have a base line for the right to health and it is impossible to cost the health service and thereby determine objectively what can be
afforded.”
We still don’t have the definition. But HIV unlike NCDs+ is a National Development Plan priority. As for the rest of the conclusions, they mostly are unmet PLWNCDs+ The main change to health services is that HIV/TB services dominate primary health care. We beg for evidence-based inclusion of NCDs + throughout the life-course. And, more not just a tack on to HIV, TB and STI services.
That is why we fight on. Read the SAHRC 2007 report on access to health services SAHRC 2007Health Report
This is billed as being about the Checka Impilo or National Wellness Campaign … but some how it got to be more about a failing health system. Take a look.
Deputy President Mabuza used the Health Summit to launch Checka Impilo, a national wellness campaign that focuses on testing and treating people who have HIV, TB, sexually transmitted infections and non-communicable diseases such as diabetes and hypertension.
The campaign will focus on the provision of comprehensive health and wellness services targeted at men, adolescent girls and young women, as well as key and vulnerable population groups.
The success of the campaign, Mabuza said, depends on coordinated collaboration among all social partners in respect to planning, implementation and monitoring.
Checka Impilo is a call to action for South Africans to move from a curative response to health to preventative approaches and the adoption of healthy lifestyles.
The campaign will focus on increased information, education and communication activities, promotion of HIV testing, widespread distribution of condoms, and provision of pre- and post-exposure prophylaxis against HIV.
“All of us must, therefore, go out in great numbers to test for HIV and screen for STIs, TB and non-communicable diseases such as diabetes and hypertension.
“Within 24 months of this campaign, we must have found and put two million more people on ARVs. We must also have found and put at least 80 000 more people with TB on anti-TB treatment. We must also have identified thousands more with diabetes, high blood pressure and cancer, and put them on treatment,” Mabuza said.
Summary: 1st WHO essential diagnostic list focusing on mainly communicable diseases with a recommendation to include more NCDs in a future edition. PHC and facility level essential package. Vicki Pinkney-Atkinson
Improving NCDs diagnosis & treatment outcomes
Today, many people are unable to get tested for diseases because they cannot access diagnostic services. Many are incorrectly diagnosed. As a result, they do not receive the treatment they need and, in some cases, may actually receive the wrong treatment.
For example, an estimated 46% of adults with Type 2 diabetes worldwide are undiagnosed, risking serious health complications and higher health costs. Late diagnosis of infectious diseases such as HIV and TB increases the risk of spread and makes them more difficult to treat.
Essential Diagnostics List (EDL)
To address this gap, WHO today published its first Essential Diagnostics List (EDL), a catalogue of the tests needed to diagnose the most common conditions as well as a number of global priority diseases.
“An accurate diagnosis is the first step to getting effective treatment ….No one should suffer or die because of a lack of diagnostic services, or because the right tests were not available.”
Dr Tedros Adhanom Ghebreyesus, WHO Director-General.
The list concentrates on in vitro tests – i.e. tests of human specimens like blood and urine. It contains 113 products: 58 tests are listed for detection and diagnosis of a wide range of common conditions, providing an essential package that can form the basis for screening and management of patients. The remaining 55 tests are designed for the detection, diagnosis and monitoring of “priority” diseases such as HIV, TB, malaria, hepatitis B and C, human papillomavirus and syphilis.
Some of the tests are particularly suitable for PHC facilities, where laboratory services are often poorly resourced and sometimes non-existent; for example, tests that can rapidly diagnose a child for acute malaria or glucometers to test diabetes. These tests do not require electricity or trained personnel. Other tests are more sophisticated and therefore intended for larger medical facilities.
“Our aim is to provide a tool that can be useful to all countries, to test and treat better, but also to use health funds more efficiently by concentrating on the truly essential tests,” says Mariângela Simão, WHO Assistant Director-General for Access to Medicines, Vaccines and Pharmaceuticals. “Our other goal is to signal to countries and developers that the tests in the list must be of good quality, safe and affordable.”
For each category of test, the EDL specifies the type of test and intended use, format, and if appropriate for primary health care or for health facilities with laboratories. The list also provides links to WHO Guidelines or publications and, when available, to prequalified products.
Similar to the WHO Essential Medicines List, which has been in use for four decades, the EDL is intended to serve as a reference for countries to update or develop their own list of essential diagnostics. In order to truly benefit patients, national governments will need to ensure appropriate and quality-assured supplies, training of healthcare workers and safe use. To that end, WHO will provide support to countries as they adapt the list to the local context.
The EDL was developed following an extensive consultation within WHO and externally. The draft list was then considered for review by WHO’s Strategic Advisory Group of Experts on In-Vitro Diagnostics – a group of 19 experts with global representation. For more information see WHO website.
WHO will update the Essential Diagnostics List on a regular basis. In the coming months, WHO will issue a call for applications to add categories to the next edition. The list will expand significantly over the next few years, as it incorporates other important areas including antimicrobial resistance, emerging pathogens, neglected tropical diseases and additional NCDs.
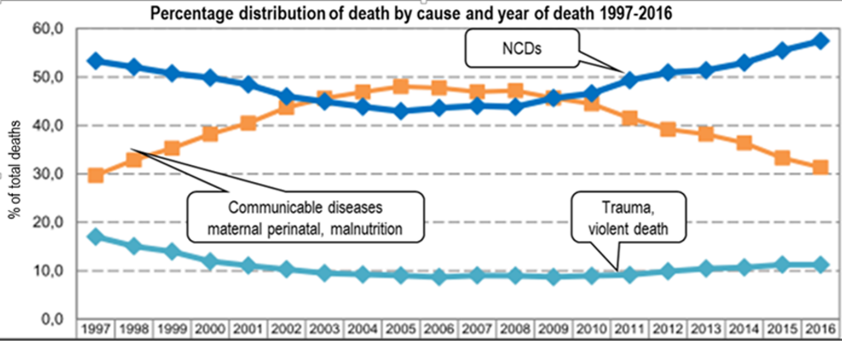
NCDs accounted for 57.4% of deaths in 2016 while communicable diseases were responsible for 31,3% of deaths. According to StatisticsSA this confirms that South Africa is in the midst of epidemiological change.
In the death stakes #1 is the position to avoid. Stroke and diabetes are the 2nd and 3rd main causes of death in South Africa according to the 2014 figures just released by StatisticsSA. TB remains in unenviable pole position but the number of deaths are dropping each year. Great news.
The ranking looks very different if diabetes and heart/ blood vessel disease are grouped. This makes sense because essentially they kill you in the same way, by cardiovascular diseases (CVD.) So this is what the figures look like done that way around
18.7% CVD (stroke, heart attacks, diabetes and other heart conditions) with <0.2% national budget and NO provincial NCDs budgets
13.2% TB & HIV/AIDS with 39.6% funding (see figure 2 right.)
Deaths from NCDs increase every year while HIV/AIDS and TB deaths have declined each year since 2007. And that is really good news. (See figure above.) However, it is disheartening that NCDs deaths continue upwards.
TB leads the number of deaths in the 15-64 age groups. The between 15-44 years infections are the big killers with HIV/AIDS in 2nd spot. NCDs don’t feature in the top ten but this changes in those over 44 year. NCDs play a much more important part.
How cost effective is screening 8 million people with diabetes and hypertension via the HIV/AIDS Counselling and Testing (HCT) programme? The stats seem to indicate different target age groups for HCT versus NCDs screening which is for at least those older than 45 years. What do you think?
The provincial ranking places the Western Cape in top CVD position followed closely by KwaZulu-Natal.

 os highlighted the problems of access to health services by millions of people living with NCDs+ in his tweet. His tweet certainly mirrors what the SA NCDs Alliance and our allies have been saying since 2007 when the SA Human Rights Commission (SAHRC) held its first public hearings into the right access to health services.
os highlighted the problems of access to health services by millions of people living with NCDs+ in his tweet. His tweet certainly mirrors what the SA NCDs Alliance and our allies have been saying since 2007 when the SA Human Rights Commission (SAHRC) held its first public hearings into the right access to health services.