The letter from the NDoH inviting 15 of the SANCDA+ members to a technical launch of the NCDs NSP on 30 June and 1 July Download the letter here All responses to Busi Nkosi View the draft programme here
Celebration time. It’s happening on 31 May 2022 in Somerset East, Eastern Cape, as part of a World No Tobacco Day event. At last, the NCDs+ civil society can breathe a collective sigh of relief. IT is the long-awaited National Department of Health’s (NDOH) NCDs+ policy for 5 years until 2027. The about-to-launched plan is a compromise, but it is way better than the early drafts. As Churchill may have said, “we are at the end of the beginning”.
If the SANCDA+ had left the NDoH decision makers to their own devices, the 3rd NCDs+ National Strategic Plan (NSP) would have been done and dusted in 2019 without credible transparency and authored mainly by a WHO Country Office appointed contractor. And that version looked remarkably similar to the previous failed 2nd NCDs plan 2013-2017. That plan wasn’t funded, implemented and only externally reviewed/evaluated in 2021.
Yes, it is the SANCDA+ activism that put a spanner in the works. Our early enthusiastic cooperation soured as it became clear that the plan would never be implemented or funded. It moved the SANCDA+ from advocacy to activism using similar tactics as HIV activists in the early part of this century. Memories are short but what is good for the goose is good for the gander.
What is different about the 3rd NCDs+ NSP? (more…)
Better late than never. And it is only until October last year. Comorbidities are published once and not routinely by NICD. Oh now, the second wave is over “we will publish another list.” Really?
This requires some myth-busting action from the National Department of Health. I am tired of the comorbidities listed in media interviews by NDoH officials as going in this order: HIV, TB and more recently malaria (really). Then perhaps diabetes…. take a look and weep. Shame
The SANCDA supports the prioritization of phase 2 vaccination. However, how this is to happen is less than transparent. PLWNCDs and related civil society organisations keep asking for transparent processes and policy for phase 2 vaccinations. South African policy must show the priority comorbid health conditions which place PLWNCDs at greatest risk for severe COVID-disease or death.
Publish – COVID-19 deaths statistics by comorbidity/ underlying conditions.
Compile – priority evidence-based list of comorbid conditions for phase 2 COVID vaccination.
Communicate with public sector “health users” in phase 2 COVID-19 vaccination
1) Publish – COVID-19 deaths stats by comorbidity
The SANCDA want the ongoing publication on COVID-19 deaths according to the main underlying comorbidities. Civil society believes the release of this information is essential for transparency. The NDoH has this information for hospitalised patients. Sadly the format of publication doesnt show linked comorbidities.
However, before COVID-19 people who die outside of a hospital, the cause of death is notoriously poorly recorded. The challenge to the data collection is a long-standing issue. The most recent report from the 2016 cause of death statistics shows that 32.5% of reported deaths has this information missing. The top category of death is NCDs in 2016 but there has not been a publication on cause of death in SA since then.
This information is critical to ensure that the limited number of doses 12 million (6 million people we think) go those in greatest need according to facts.
The challenge is that outside of the NCDs sub directorate, the NDoH does not respond to our many requests for information. The NCDs civil society experience is that the long-held NDoH priority conditions of HIV, TB and malaria always remain just that. NCDs may get a mention and usually only diabetes and hypertension. So we want all of society to ask on behalf of the people living with NCDs.
2) Compile priority evidence-based list of comorbid conditions
So far in this pandemic we havent seen any transparent evidence based list of priority comorbid conditions. So how is this the priority to be determined? Compared with Millenium Development Goal (MDG) conditions like HIV/TB there are few NCDs indicators as shown in the National Indicator Data Set 2016.
South African health policy appears to be silent on how health priorities are determined. One of the few policies that address the needs of the population (priorities) is still in draft format and relatively recent, NHI Bill 2019.
PLWNCDs and their representative organisations wish to participate in and have a transparent evidence-based process to determine priority need and the criteria upon which this is based.
3) Communicate unambiguously with public sector users
The SANCDA asks for transparent clear communication on how people without health insurance/ medical aid will be selected and notified of vaccination date and time. There are no adequate health systems information for people with NCDs. The current NHI health systems information is based on HIV and MDG information. MDG conditions formed the basis for the development of health systems strengthening information system development and programmes such as the “Ideal Clinic.” integrated chronic disease management and CCMDD are all examples. See the CCMDD access to medicines information and raise a storm.
It is our third week of hosting the #diabetes helpline. One clear message is that access to #insulin and other supplies are problematic in the public sector for those with #type1diabetes or #type2diabetes.
Insulin is injected and must be administered as prescribed and on time. Skipping doses or cutting back can have fatal consequences within a short time. The chronic neglect of #NCDs in the South African public health sector means that inulin is seldom available at a primary health care clinic. Meaning one has to go to a higher level of care to get supplies. This means a trip to a community health centre or hospital. Let’s just make it difficult for diabetics.
For the patient, this involves greater risks of lengthy taxi trips and waiting periods in crowded hospitals. What a way to treat people with pre-existing “underlying” health problems! Also known as #NCDs ! We are at the greatest risk of dying from severe #covid19 illness.
I am in awe of the creative ways that our empowered patients are getting medicines without standing in queues or travelling for a day. Pure survival instincts at work. We salute the private #phamacies that filled prescriptions in the national lockdown. And then, there are the unsung heroes who shared their meds because they know what happens if … #equity
The National Department of Health’s central chronic medicines dispensing and distribution programme, #CCMDD, must be urgently extended to all common #NCDs including insulin. For over a year we have asked the statistics for NCDs medicines supply using CCMDD. #transparency #equity #accountability
What does proof of concept for CCMDD NCDs look like? A verifiable table showing:
NCDs conditions treated
NCDs medicines and supplies formulary
Clinics and district involved
The number of NCDs patients registered by the clinic.
Timelines for full rollout.
Insulin is at the top of that list. We are still waiting. #COVID19 pandemic shows just why the health systems strengthening goes beyond #TB and #HIV
Reading the Auditor General’s report 2018-19 is not the way to finish off a week. It is a dismal tale of woe which adds another distressing layer to the state capture saga. What is truly distressing is that this information is in plain sight and very little is done from one year to the next. The Citizens version candidly spells it out: “overall audit outcomes take a turn for the worse over five years.” For me, it is much clearer that the boffins’ version of the report which sugar coats the message as “audit outcomes regressed since 2014/15.”
Provincial departments of health are in a bad state and need urgent intervention to prevent collapse. An exception is the Western Cape.
Serious weaknesses in the financial management of national & provincial government unaddressed in the last five years. (Section 4)
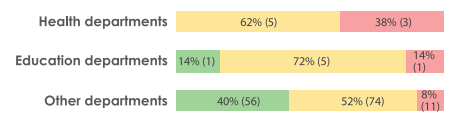
The quality of the performance reports slightly regressed since 2014/15 from 66% to 62% (auditees publishing credible reports).
Little improvement on key government programmes according to the National Development Plan Section 6 district health services (HIV/AIDS, TB &maternal & child health) box below water infrastructure development, housing development finance, school infrastructure delivery expanded public works programme.
72% of the auditees materially did not comply with legislation similar to the previous year & slightly higher than the 70% in 2014/15.
What does this mean for National Health Insurance Bill and sweeping changes needed for the financing of health care? The National Department of Health is not among those that received a clean (unqualified) audit.

 Celebration time. It’s happening on 31 May 2022 in Somerset East, Eastern Cape, as part of a World No Tobacco Day event. At last, the NCDs+ civil society can breathe a collective sigh of relief. IT is the long-awaited National Department of Health’s (NDOH) NCDs+ policy for 5 years until 2027. The about-to-launched plan is a compromise, but it is way better than the early drafts. As Churchill may have said, “we are at the end of the beginning”.
Celebration time. It’s happening on 31 May 2022 in Somerset East, Eastern Cape, as part of a World No Tobacco Day event. At last, the NCDs+ civil society can breathe a collective sigh of relief. IT is the long-awaited National Department of Health’s (NDOH) NCDs+ policy for 5 years until 2027. The about-to-launched plan is a compromise, but it is way better than the early drafts. As Churchill may have said, “we are at the end of the beginning”.